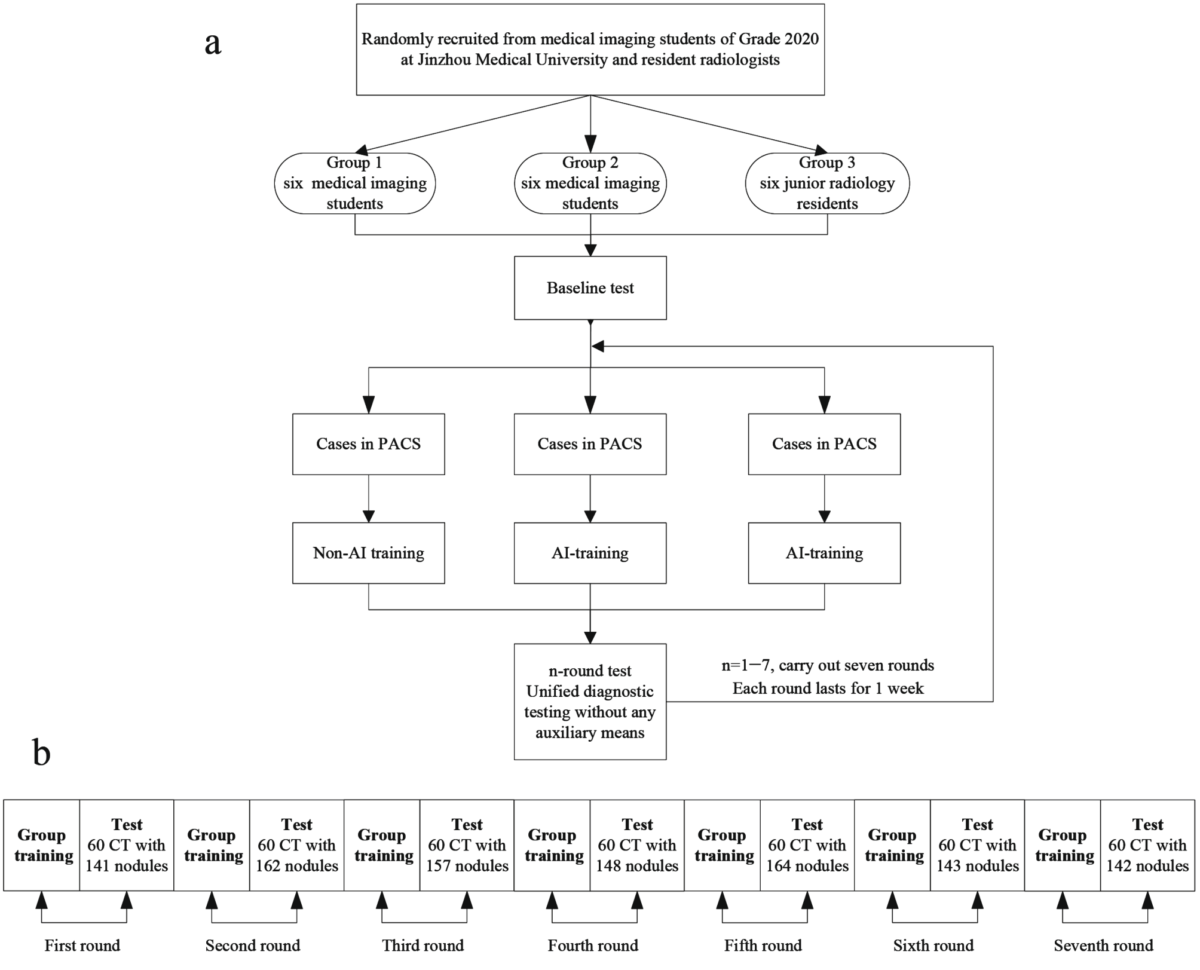
Group design
Members had been randomly recruited from amongst first-year radiology residents and medical imaging students coming into medical research on the Jinzhou Medical College. Based mostly on totally different strategies of image training, they had been divided into three teams. Group 1: six five-year medical imaging students of Grade 2020 who learn footage independently with the image archiving and communication system (PACS). Group 2: six five-year medical imaging students of Grade 2020 who learn footage with AI. Group 3: six junior radiology residents who learn footage with AI. Teams 1 and 2 had not too long ago accomplished the theoretical studying of lung imaging prognosis earlier than enrollment. Earlier than the training, all individuals within the three teams participated within the check associated to lung nodule imaging efficiency. The scores in Teams 1, 2 and 3 had been (77.50 ± 8.17), (80.33 ± 7.92) and (89.33 ± 4.50), respectively. There was no statistical distinction between Teams 1 and 2(P > 0.05). Nevertheless, the distinction between the primary two teams and the third group was statistically important (P = 0.036 and 0.011).
Traing and check
Within the non-AI training mode (Group 1), lecturers summarised the prognosis factors and circumstances of pulmonary nodules in 10–15 min. Subsequent, circumstances pushed to the PACS, the place students learn photographs in teams and participated in dialogue and prognosis. Lastly, they rectified errors based mostly on comparability with customary case experiences.
Within the AI-training mode (Teams 2 and 3), lecturers summarised the prognosis factors and circumstances of pulmonary nodules in 10–15 min; thereafter, the students used AI for sensible training. First, the operators learn and identified the circumstances independently utilizing the PACS. Subsequent, the AI software program was used to accumulate and summarise the detailed data marked on the software program, corresponding to nodules and lesions, particular positions of lung lobes and lung segments, and the judgment of benign and malignant tumors. Lastly, group discussions had been carried out to deal with any misunderstandings or doubts, after which, the lecturers addressed students’ queries.
The length of every spherical was one week (two class hour/day); that of your complete course of was seven weeks. Determine 1a illustrates the analysis flowchart.
A complete of 420 plain computed tomography (CT) photographs with 1,057 pulmonary nodules had been included within the check, which was carried out for seven rounds with 60 photographs per spherical. Every spherical incorporates benign and malignant nodules. All three teams underwent checks with none auxiliary circumstances (Fig. 1b). Inclusion standards: (1) 1 ≤ quantity of pulmonary nodules per case ≤ 5; (2) Nodules with diameter between 3 and 30 mm [10]; and (3) Thickness of CT-reconstructed picture 1 mm. Exclusion standards: (1) Diffuse lung lesions; (2) Earlier pulmonary surgical procedure historical past; (3) A number of lung metastases; and (4) Artifacts or falling results within the photographs.
Observations and grading strategies
The diameter, form, edge, density, boundary, vacuole or cavity, lobulation signal, pleural despair signal, vascular cluster signal and different indicators of pulmonary nodules had been noticed. Based mostly on the indicators, benign and malignant prognosis was made. Prognosis of pulmonary nodules was graded in response to the Lung CT Screening Reporting and Information System [11, 12] (Lung-RADS) (Desk 1).
Classification and standards
Based mostly on the density of pulmonary nodules [13], they had been categorized into stable nodule (a nodule that fully covers the lung parenchyma), purely floor glass nodule (pGGN) (a hazy opacity with out blocking underlying pulmonary vessels or bronchial construction, no stable parts), combined floor glass nodule (mGGN) (a nodule with floor glass parts in addition to stable parts) and calcified nodule (a nodule with calcium deposition). Based mostly on the situation of pulmonary nodules, they had been categorized into subpleural nodules (related to the pleura), central nodules (inside 20 mm of the hilar), and peripheral nodules (outdoors the hilar area, however not related to the pleura). Based mostly on the utmost diameter of nodules, they had been divided into small nodules (lower than 5 mm), medium nodules (5 to 10 mm), and massive nodules (over 10 mm).
Two affiliate chief physicians with 10 years of expertise in chest imaging noticed, recognized and marked the lesions by referring to AI outcomes on the skinny part CT photographs (1 mm), judged the categories of nodules, recorded the dimensions of nodules, and thereafter, ascertained the authenticity of nodules utilizing the multi-planar reconstruction and most density projection know-how. The consensus of the 2 medical doctors and the typical dimension of nodules had been taken because the reference customary. In case of totally different opinions, the senior doctor shall be invited to seek the advice of for affirmation. For nodules with surgical procedure or puncture, pathological findings had been the standards. For nodules with out pathological outcomes, the diagnostic opinions of radiologists had been the standards. Detection fee = (quantity of true optimistic nodules/complete quantity of nodules) ×100%. Prognosis coincidence fee = (quantity of appropriately identified nodules /complete quantity of nodules) ×100%. False optimistic quantity/every case = quantity of false optimistic nodules/quantity of circumstances.
Introduction to the AI-assisted prognosis system
AI movie studying was carried out utilizing the medical clever picture assisted prognosis software program (V4.0 model) of the Beijing Medical Clever Know-how Co., LTD. The efficiency of AI alone on check datasets was as follows: sensitivity of 95.3%, specificity of 96.8%. When the entire authentic CT photographs are imported into the system, the lung picture information will be labelled in batches and may routinely delineate the area of curiosity to routinely find, measure and diagnose the pulmonary nodules. In the appropriate column of the system interface, the quantity of pulmonary nodules, degree, diameter, kind, location and malignancy of every nodule may very well be displayed (Fig. 2). Subsequent, a whole AI report will be issued, which may very well be pushed to the PACS terminal with one click on. The system may independently choose the longest diameter vary of displayed nodules so as to add or delete nodules, as required. Because the inclusion standards of this examine, it’s set to detect and diagnose solely the nodules with diameter between 3 and 30 mm.

AI assisted prognosis system interface. (a) The marking interface of AI assisted system that may show the situation, amount, kind, and grading. data of lung nodules. (b) The measurement interface of the system, which additional shows the quantity and dimension of nodules based mostly on a
Statistical evaluation
The SPSS 23.0 (IBM, Chicago, USA) software program was used for statistical evaluation, and GraphPad Prism 8.0 (GraphPad, California, USA) was used for information plotting. Tree prognosis classifications had been set as with/with out pulmonary nodule, and benign/malignant nodule. The detection fee, diagnostic compliance fee and false optimistic quantity/case of every group had been calculated. The counting information had been expressed as % and the χ2 check was used for comparability among the many teams. Measurements with regular distribution had been expressed as imply ± customary deviation ((mathop {rm X}limits^ – ; pm ;{rm{s}})), and the T-test, F-test had been carried out for inter-group and multi-group comparisons. The Kappa rating was used to judge the intra-group consistency of the check outcomes of every spherical for three teams of trainees, which had been calculated by combining the typical worth of the harmonic of the three classifications. The kappa scores between 0.41 and 0.60 had been thought-about common settlement, between 0.61 and 0.80 had been thought-about important settlement, and above 0.80 had been thought-about extremely settlement. The distinction was statistically important with P < 0.05.